

26 May Mobile Dual-Energy X-ray: Improving Imaging Where Access is a Challenge

KA Imaging’s Reveal 35C is a solution for better mobile imaging – especially in challenging environments like the ER. The Reveal 35C X-ray detector provides high-quality DR images (up to 75% DQE), with the added benefit of offering dual-energy images in mobile applications. It uses the same dose, same source and same workflow as a regular X-ray. Reveal’s dual-energy images can be used for better visualization of line and tube tips, retained surgical objects, pneumothorax, bedside pneumonia, among other applications. Read this interview with KA Imaging’s CTO Dr. Karim S Karim to learn more.
What is the difference between a mobile dual-energy X-ray system and a mobile or fixed regular X-ray system?
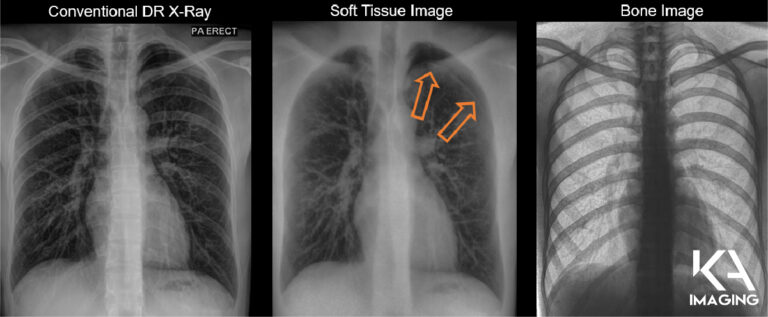
Karim S. Karim, CTO of KA Imaging: The biggest difference with dual energy is that you get better discrimination of soft tissue and bone. With the Reveal 35C technology we’re getting a regular X-ray, plus a soft tissue image and a bone image. The advantage of these spectral images, the soft tissue and the bone, is that you can visualize soft tissue without interference from the bone. You can visualize bone without interference from the soft tissue. For example: in the bone image you can see lines, tubes and calcified nodules beautifully; in the soft tissue image you can see pneumothorax and pneumonia quite nicely.
 You also have patients in long term care facilities, some experiencing mobility issues, they can’t really go around to be imaged. Imaging must go to them.
You also have patients in long term care facilities, some experiencing mobility issues, they can’t really go around to be imaged. Imaging must go to them.
Another interesting use case is prisons. If you’re trying to do any kind of screening of disease there, you can’t very well take a CT to that patient. So again, a portable solution is where the value comes in.
Screening or triaging for general population is also an interesting application. If you’re trying to triage cardiac disease or lung cancer or tuberculosis or even pulmonary fibrosis… Any other kind of occupational health disease. In those situations, using CT is not the right solution because the radiation dose is very high and if you’re screening such a large general population, the radiation dose to that population will be unacceptable. Even with LDCT, you are still looking at 10X to 20X more radiation than a standard AP X-ray so the ALARA principle would guide us to use the lowest dose modality that can provide a good outcome. There is also a limitation in terms of access to LDCT as well as infrequent follow ups because patients are concerned about CT dose, as we know… In those situations, a mobile Reveal system again can be quite valuable. Because it’s mobile, because it’s portable, it can be used in screening centers that are distributed across, without having to be concentrated just in hospitals. There could be units in long term care facilities, they could be in mobile vans, they could be in rural and remote areas… And that’s where the screening element becomes quite valuable.
What is the impact for rural and remote communities?
KK – The biggest challenge for these communities is access. The second piece that’s challenging for these communities is not just access to equipment, but also access to qualified radiologists, qualified clinicians to make a timely diagnosis. So even though one could argue that we can send the images to be read overseas or to be read using teleradiology, the question is in some situations you need a diagnosis instantly. For example, if I’m in a rural community in the ICU and I’ve got a pneumothorax, I need that diagnosis immediately because waiting for three hours may cause a very serious change in the patient condition.
These are also situations where spectral imaging combined with, for example, some kind of artificial intelligence or computer aided diagnosis could enable an instant diagnosis. It’s something that regular X-ray couldn’t do because it doesn’t have that material classification and identification capability that spectral imaging does. So it’s not just about access to equipment, it’s also access to a timely diagnosis.